Tetralogy of Fallot
Tetralogy (teh-TRAL-o-je) of Fallot (fah-LO) is a congenital heart defect. A congenital heart defect is a problem with the heart's structure that's present at birth. This type of heart defect changes the normal flow of blood through the heart.
Tetralogy of Fallot is a rare, complex heart defect that occurs in about 5 out of every 10,000 babies. It affects boys and girls equally.
To understand this defect, it's helpful to know how a healthy heart works. The Diseases and Conditions Index How the Heart Works article describes the structure and function of a healthy heart. The article also has animations that show how your heart pumps blood and how your heart's electrical system works.
Overview
Tetralogy of Fallot involves four heart defects:
- A large ventricular septal defect (VSD)
- Pulmonary (PULL-mon-ary) stenosis
- Right ventricular hypertrophy (hi-PER-tro-fe)
- An overriding aorta
Ventricular Septal Defect
The heart has a wall that separates the two chambers on its left side from the two chambers on its right side. This wall is called a septum. The septum prevents blood from mixing between the two sides of the heart.
A VSD is a hole in the part of the septum that separates the ventricles, the lower chambers of the heart. The hole allows oxygen-rich blood from the left ventricle to mix with oxygen-poor blood from the right ventricle.
Pulmonary Stenosis
This defect is a narrowing of the pulmonary valve and the passage through which blood flows from the right ventricle to the pulmonary artery.
Normally, oxygen-poor blood from the right ventricle flows through the pulmonary valve, into the pulmonary artery, and out to the lungs to pick up oxygen. In pulmonary stenosis, the heart has to work harder than normal to pump blood, and not enough blood reaches the lungs.
Right Ventricular Hypertrophy
This defect occurs if the right ventricle thickens because the heart has to pump harder than it should to move blood through the narrowed pulmonary valve.
Overriding Aorta
This is a defect in the aorta, the main artery that carries oxygen-rich blood to the body. In a healthy heart, the aorta is attached to the left ventricle. This allows only oxygen-rich blood to flow to the body.
In tetralogy of Fallot, the aorta is between the left and right ventricles, directly over the VSD. As a result, oxygen-poor blood from the right ventricle flows directly into the aorta instead of into the pulmonary artery to the lungs.
Outlook
Together, these four defects mean that not enough blood is able to reach the lungs to get oxygen, and oxygen-poor blood flows out to the body.
Normal Heart and Heart With Tetralogy of Fallot
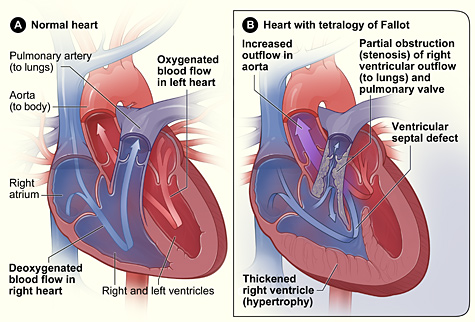
Figure A shows the structure and blood flow in the interior of a normal heart. Figure B shows a heart with the four defects of tetralogy of Fallot.
Babies and children who have tetralogy of Fallot have episodes of cyanosis (si-a-NO-sis). This is a bluish tint to the skin, lips, and fingernails. Cyanosis occurs because the oxygen level in the blood is below normal.
Tetralogy of Fallot must be repaired with open-heart surgery, either soon after birth or later in infancy. The timing of the surgery depends on how severely the pulmonary valve is narrowed.
Over the past few decades, the diagnosis and treatment of tetralogy of Fallot have greatly improved. As a result, most children who have this heart defect survive to adulthood. However, they'll need lifelong medical care from specialists to help them stay as healthy as possible.
Other Names for Tetralogy of Fallot
- Fallot's tetralogy
What Causes Tetralogy of Fallot?
Doctors don't know what causes most cases of tetralogy of Fallot and other congenital heart defects.
Certain conditions or factors that occur during pregnancy may raise your risk for having a child with tetralogy of Fallot. These conditions and factors include:
- German measles (rubella) and some other viral illnesses
- Poor nutrition
- Overuse of alcohol
- Age (being older than 40)
- Diabetes
Heredity may play a role in causing tetralogy of Fallot. An adult who has tetralogy of Fallot may have an increased chance of having a baby with the condition.
Children who have certain genetic disorders, such as Down syndrome and DiGeorge syndrome, often have congenital heart defects, including tetralogy of Fallot.
Scientists continue to search for the causes of tetralogy of Fallot and other congenital heart defects.
What Are the Signs and Symptoms of Tetralogy of Fallot?
An important sign of tetralogy of Fallot is cyanosis. Cyanosis is a bluish tint to the skin, lips, and fingernails. Low levels of oxygen in the blood cause cyanosis.
Babies who have unrepaired tetralogy of Fallot sometimes have "tet spells" in response to an activity like crying or having a bowel movement. A tet spell occurs when the oxygen level in the blood suddenly drops. This causes the baby to become very blue. The baby also may:
- Have a hard time breathing
- Become very tired and limp
- Not respond to a parent's voice or touch
- Become very fussy
- Lose consciousness
In years past, when tetralogy of Fallot wasn't treated in infancy, children would get very tired during exercise and could faint. This heart defect is now repaired in infancy to prevent symptoms like this.
Another common sign of tetralogy of Fallot is a heart murmur. A heart murmur is an extra or unusual sound that doctors may hear while listening to the heart.
The sound occurs because the heart defect causes abnormal blood flow through the heart. However, not all heart murmurs are signs of congenital heart defects. Many healthy children have heart murmurs.
Normal growth and development depend on a normal workload for the heart and normal flow of oxygen-rich blood to all parts of the body. Babies who have tetralogy of Fallot may not gain weight or grow as quickly as children who have healthy hearts because they tire easily while feeding.
Children who have tetralogy of Fallot also may have clubbing. Clubbing is the widening or rounding of the skin or bone around the tips of the fingers.
How Is Tetralogy of Fallot Diagnosed?
Doctors diagnose tetralogy of Fallot based on a baby's signs and symptoms, a physical exam, and the results from tests and procedures.
Signs and symptoms of the heart defect usually occur during the first weeks of life. Your infant's doctor may notice signs or symptoms during a routine checkup. Some parents also notice cyanosis (a bluish tint to the skin, lips, and fingernails) or poor feeding and bring the baby to the doctor.
Specialists Involved
If your child has tetralogy of Fallot, a pediatric cardiologist and cardiac surgeon may be involved in his or her care.
A pediatric cardiologist is a doctor who specializes in diagnosing and treating heart problems in children. Cardiac surgeons repair heart defects using surgery.
Physical Exam
During a physical exam, the doctor may:
- Listen to your baby's heart and lungs with a stethoscope.
- Look for signs and symptoms, such as a bluish tint to the skin, lips, or fingernails and rapid breathing.
- Look at your baby's general appearance. Some children who have tetralogy of Fallot have characteristic facial traits because they have DiGeorge syndrome.
Diagnostic Tests and Procedures
Your child's doctor may recommend several tests to diagnose tetralogy of Fallot. These tests can provide information about the four heart defects that occur in tetralogy of Fallot and how serious they are.
Echocardiography
Echocardiography (echo) is a painless test that uses sound waves to create a moving picture of the heart. During the test, the sound waves (called ultrasound) bounce off the structures of the heart. A computer converts the sound waves into pictures on a screen.
Echo allows the doctor to clearly see any problem with the way the heart is formed or the way it's working.
Echo is an important test for diagnosing tetralogy of Fallot because it shows the four heart defects and how the heart is responding to them. This test helps the cardiologist decide when to repair these defects and what type of surgery is needed.
Echo also is used to check a child's condition over time, after the defects have been repaired.
EKG (Electrocardiogram)
An EKG is a simple, painless test that records the heart's electrical activity. The test shows how fast the heart is beating and its rhythm (steady or irregular). It also records the strength and timing of electrical signals as they pass through each part of the heart.
An EKG also can help the doctor determine whether the right ventricle is enlarged (ventricular hypertrophy).
Chest X Ray
A chest x ray is a painless test that creates pictures of the structures in the chest, such as the heart and lungs. This test can show whether the heart is enlarged or whether the lungs have extra blood flow or extra fluid, a sign of heart failure.
Pulse Oximetry
For this test, a small sensor is attached to a finger or toe (like an adhesive bandage). The sensor gives an estimate of how much oxygen is in the blood.
Cardiac Catheterization
During cardiac catheterization (KATH-e-ter-i-ZA-shun), a thin, flexible tube called a catheter is put into a vein in the arm, groin (upper thigh), or neck and threaded to the heart.
Special dye is injected through the catheter into a blood vessel or a chamber of the heart. The dye allows the doctor to see the flow of blood through the heart and blood vessels on an x-ray image.
The doctor also can use cardiac catheterization to measure the pressure and oxygen level inside the heart chambers and blood vessels. This can help the doctor determine whether blood is mixing between the two sides of the heart.
How Is Tetralogy of Fallot Treated?
Tetralogy of Fallot must be repaired with open-heart surgery, either soon after birth or later in infancy. The goal of surgery is to repair the four defects of tetralogy of Fallot so the heart can work as normally as possible. Repairing the defects can greatly improve a child's health and quality of life.
The pediatric cardiologist and cardiac surgeon will decide the best time to do the surgery. Their decision will be based on your baby's health and weight, how severe the defects are, and how severe your baby's symptoms are.
Sometimes, teenagers or adults who had tetralogy of Fallot repaired in childhood need additional surgery to correct heart problems that develop over time. See "Living With Tetralogy of Fallot" for more information.
Types of Surgery
Complete Intracardiac Repair
Surgery to repair tetralogy of Fallot is done to improve blood flow to the lungs and to make sure that oxygen-rich and oxygen-poor blood flows to the right places. The surgeon will:
- Widen the narrowed pulmonary blood vessels. The pulmonary valve is widened or replaced, and the passage from the right ventricle to the pulmonary artery is enlarged. These procedures improve blood flow to the lungs. This allows the blood to get enough oxygen to meet the body's needs.
- Close the ventricular septal defect (VSD). A patch is used to cover the hole in the septum. This patch stops oxygen-rich and oxygen-poor blood from mixing between the ventricles.
Fixing these two defects resolves problems caused by the other two defects. When the right ventricle no longer has to work so hard to pump blood to the lungs, it will return to a normal thickness. Fixing the VSD means that only oxygen-rich blood will flow out of the left ventricle into the aorta.
The incision (cut) that the surgeon makes to reach the heart usually heals in about 6 weeks. The surgeon or a hospital staff member will explain when it's okay to give your baby a bath, pick him or her up under the arms, and take your baby for his or her regular shots (immunizations).
Temporary or Palliative Surgery
It was common in the past to do temporary surgery during infancy in babies who had tetralogy of Fallot. This surgery improved blood flow to the lungs. A complete repair of the four defects was done later in childhood.
Now, most babies who have tetralogy of Fallot have their defects fully repaired in infancy. However, some babies are too weak or too small to have the full repair. They must have temporary surgery first. This surgery improves oxygen levels in the blood. It also gives the baby time to grow and get strong enough for the full repair.
In the temporary surgery, the surgeon places a tube called a shunt between a large artery branching off the aorta and the pulmonary artery. One end of the shunt is sewn to the artery branching off the aorta. The other end is sewn to the pulmonary artery.
The shunt creates an additional pathway for blood to travel to the lungs to get oxygen. The shunt is removed when the baby's heart defects are fixed during the full repair.
After temporary surgery, your baby may need medicines to keep the shunt open while waiting for the full repair. These medicines are stopped after the shunt is removed.
Living With Tetralogy of Fallot
The outlook for a child born with tetralogy of Fallot is much better today than in the past. Advances in testing and treatment mean that most children who have this congenital heart defect survive to adulthood. However, they need long-term care from specialists to stay as healthy as possible.
Caring for Your Child at Home
Feeding and Nutrition
Babies who have tetralogy of Fallot can tire while nursing or feeding. Small, frequent meals may be easier for your baby to handle.
Your child also may need extra nutrition. A supplement or an extra feeding can give the baby more calories, vitamins, or iron. Your child's doctors will work with you to determine what extra nutrition your baby needs.
Tet Spells
"Tet spells" can occur in babies whose tetralogy of Fallot hasn't yet been repaired. Lowering your baby's anxiety or stress can help prevent tet spells and save the baby's energy. For example, slowly picking up your baby and speaking in a soothing voice can avoid startling him or her, which may prevent or reduce crying.
Talk to your doctor about how you can manage your child's tet spells. Your doctor may suggest that you:
- Bring the child's knees up tight against his or her chest (this is called the knee-chest position) or have your child squat down. This will increase blood flow to the lungs.
- Try to calm your child.
- Call 9-1-1 if the symptoms don't improve right away.
Activity Restrictions
Some children who have tetralogy of Fallot may need to limit certain types of physical activity. The limits vary with each child. Talk to your child's doctor about whether:
- Your child needs to restrict activity or exercise
- Your child can play in organized sports, especially contact sports
- You need a note for your child's school or coaches about limiting your child's exercise
Ongoing Medical Care
Children who have tetralogy of Fallot should have ongoing medical care. This includes:
- Seeing a pediatric cardiologist for heart checkups as directed
- Seeing a pediatrician or family health care provider for routine exams
- Making sure your child takes medicines as prescribed
Children who have severe heart defects, like tetralogy of Fallot, may be at slightly increased risk for infective endocarditis (IE). IE is a serious infection of the inner lining of your heart chambers and valves.
In a few situations, your child's doctor or dentist may give your child antibiotics before medical or dental procedures (such as surgery or dental cleanings) that could allow bacteria into the bloodstream. Your child's doctor will tell you whether your child needs to take antibiotics before such procedures.
To reduce the risk of IE, gently brush your young child's teeth every day as soon as they begin to come in. As your child gets older, make sure he or she brushes every day and sees a dentist regularly. Talk with your child's doctor and dentist about how to keep your child's mouth and teeth healthy.
Consider having your child wear a medical alert bracelet or necklace. This alerts anyone caring for your child that the child has tetralogy of Fallot.
You may want to work with your health care providers to put together a packet of medical records and information that covers all aspects of your child's heart defect, including:
- Diagnosis
- Procedures or surgeries
- Prescribed medicines
- Recommendations about medical followup and how to prevent complications
- Health insurance
Keeping your health insurance current is important. For example, if you plan to change jobs, find out whether your new health insurance will cover care for your child's congenital heart defect.
Some health insurance plans may not cover medical conditions that were covered under a previous plan.
Special Needs for Teenagers and Adults
As children who have tetralogy of Fallot grow up and become teens, it's important that they understand the condition, how it was treated, and what kind of care may still be needed.
This understanding will help them take responsibility for their health. It also will help ensure a smooth transition when they start getting care from a cardiologist instead of a pediatric cardiologist. A cardiologist treats adults who have heart problems.
It's also very important for teens to have health insurance as adulthood approaches. Review your current health insurance plan. Find out whether you can extend coverage to your child beyond the age of 18. Some policies may allow you to keep your child on your plan if he or she remains in school or is disabled.
Some teenagers or young adults need additional surgery. For example, the pulmonary valve can narrow again over time, reducing blood flow. The valve may need to be widened or replaced. The cardiologist will discuss with you and your teenager the need for any additional heart surgeries.
Over time, people who have had surgery to repair tetralogy of Fallot also may face a number of other heart problems.
Leaking Heart Valves
The heart has four valves that open and close with each heartbeat. These valves ensure that blood flows in only one direction.
If a valve doesn't seal tightly, blood can leak back into the chamber it came from. This is called backflow or regurgitation (re-GUR-ji-TA-shun), and it can lead to symptoms and complications.
The most frequent problem that occurs after tetralogy of Fallot repair is pulmonary backflow, or leaking from the pulmonary valve. Backflow from the tricuspid valve and aortic valve also can occur. Surgery is needed to repair or replace the leaking valve.
Arrhythmias
Arrhythmias (ah-RITH-me-ahs) are another complication that may develop. Arrhythmias are problems with the rate or rhythm of the heartbeat.
Arrhythmias linked to tetralogy of Fallot include ventricular tachycardia, atrial fibrillation, and atrial flutter. For more information, see "Types of Arrhythmia."
Medicines are used to control these arrhythmias. Medical procedures or surgery also may be needed to treat arrhythmias.
Pulmonary Artery Branch Stenoses
Over time, the pulmonary valve can narrow again. This will reduce blood flow to the lungs, making the heart work harder than it should. Several surgical techniques can be used to fix this problem.
Right Ventricular Aneurysms
The patch used to fix the ventricular septal defect (VSD) can cause areas of the ventricle to weaken. The areas, called aneurysms (AN-u-risms), can bulge or "balloon" out.
Aneurysms make it hard for the heart to function as well as it should. This problem must be repaired with surgery.
Residual Ventricular Septal Defects
Sometimes, VSDs still leak even after they've been repaired. VSDs are repaired again if they're large or are causing problems with the function of the right ventricle.
Coronary Heart Disease
As people who have repaired tetralogy of Fallot approach middle age, they can develop coronary heart disease (CHD), just as adults who don't have heart defects can.
CHD, also called coronary artery disease, is a condition in which a fatty substance called plaque (plak) builds up in the coronary (heart) arteries. CHD can lead to chest pain, shortness of breath, and heart attack.
Preventing CHD is especially important because the procedures done to relieve CHD, like coronary artery bypass grafting, can cause complications in people who have repaired tetralogy of Fallot.
Other Considerations
Many women with repaired tetralogy of Fallot who become pregnant are able to have successful, full-term pregnancies. Others may have difficult pregnancies.
Women with tetralogy of Fallot who want to become pregnant (or who are pregnant) should talk to their doctors about:
- Health risks during pregnancy
- Medicines they can take during pregnancy
- Any new or worsening symptoms
These women also should consult specialists who take care of pregnant women who have heart conditions, such as congenital heart defects.
Adults who were born with tetralogy of Fallot should consider job changes carefully, because health benefits may change. Some health plans have waiting periods or clauses to exclude some types of coverage. Before making any job changes, find out whether the change will affect your health insurance.
Several laws protect the employment rights of people who have health conditions, such as congenital heart defects. The Americans with Disabilities Act and the Work Incentives Improvement Act try to ensure fairness in hiring for all people, including those who have health conditions.
Key Points
- Tetralogy of Fallot is a rare, complex congenital heart defect. A congenital heart defect is a problem with the heart's structure that's present at birth.
- Tetralogy of Fallot involves four heart defects:
- A large ventricular septal defect (VSD)
- Pulmonary stenosis
- Right ventricular hypertrophy
- An overriding aorta
- Together, these four defects mean that not enough blood is able to reach the lungs to get oxygen, and oxygen-poor blood flows out to the body.
- Doctors don't know what causes most cases of tetralogy of Fallot. Certain conditions or factors that occur during pregnancy may raise your risk for having a child with tetralogy of Fallot. Heredity and some genetic disorders also may play a role in causing this condition.
- An important sign of tetralogy of Fallot is cyanosis. Cyanosis is a bluish tint to the skin, lips, and fingernails. Other signs and symptoms include a heart murmur, delayed growth and development, and clubbing. Clubbing is the widening or rounding of the skin or bone around the tips of the fingers.
- Babies who have unrepaired tetralogy of Fallot sometimes have "tet spells." A tet spell occurs when the oxygen level in the blood suddenly drops. This causes the baby to become very blue. He or she also may have trouble breathing, become very tired and limp, not respond to a parent's voice or touch, become very fussy, or lose consciousness.
- Doctors diagnose tetralogy of Fallot based on a baby's signs and symptoms, a physical exam, and the results from tests and procedures. Signs and symptoms of the heart defect usually occur during the first weeks of life.
- Tetralogy of Fallot must be repaired with open-heart surgery, either soon after birth or later in infancy. The goal of surgery is to repair the four defects of tetralogy of Fallot so the heart can work as normally as possible.
- Surgery involves widening or replacing the pulmonary valve and enlarging the passage from the right ventricle to the pulmonary artery. This improves blood flow to the lungs. Surgeons also close the VSD with a patch. The patch stops oxygen-rich and oxygen-poor blood from mixing between the ventricles. Fixing these two defects resolves problems caused by the other two defects.
- Some babies who are very small or weak have a temporary procedure that improves blood flow to the lungs and gives the baby time to grow and get strong enough for the full repair.
- Advances in treatment mean that most children who are born with tetralogy of Fallot survive to adulthood. However, these children need lifelong care from specialists to stay as healthy as possible.
- Teenagers and adults who had surgery to repair tetralogy of Fallot may have long-term heart problems, such as heart function problems, arrhythmias (irregular heartbeats), or problems resulting from the original repair. These problems are treated with medicines, procedures, and surgery.


